Maternal and Child Health Today
Reducing maternal and child mortality in vulnerable populations has become a priority in global health. Despite achievements in improving the health of mothers and children under five, new approaches are needed to ensure more progress is made. In 2000, the Millennium Development Goals (MDGs) were established with the aim of reducing maternal and child mortality rates by three-fourths by 2015. The majority of countries have not achieved such success, especially in sub-Saharan Africa, where only five of 44 countries are on track.* Progress has been stunted due to the low population coverage of key interventions proven to be effective in reducing mortality. There is a lack of evidence that facility-based services alone can achieve high levels of coverage in resource-limited areas with high mortality rates.
The Care Group approach uses lower-level paid workers, volunteers, and community household members to share vital messages with mothers and promote important health behaviors and key health services. Care Groups use volunteers to motivate mothers to adopt life-saving maternal and child health behaviors. This approach emphasizes peer-to-peer health promotion, selection of volunteers by the mothers, frequent contact between volunteers and mothers, and regular supervision of the volunteers.*
What is a Care Group?
Community Health Workers (CHW) are widely used in global health interventions and are successful in engaging community members and spreading health education. CHWs work within the health system at the community level outside of health facilities. Some CHW programs have been credited with achieving high levels of population coverage in maternal and child health programs and in improving child survival. Care Groups build on the idea of CHWs, but rely on volunteer CHWs to expand coverage of maternal and child health interventions. The incorporation of volunteers allows health programs to reach a great population without increasing overall program costs. Engaging community members as volunteers also creates community ownership and increases the sustainability of the program.*
Care Group Structure
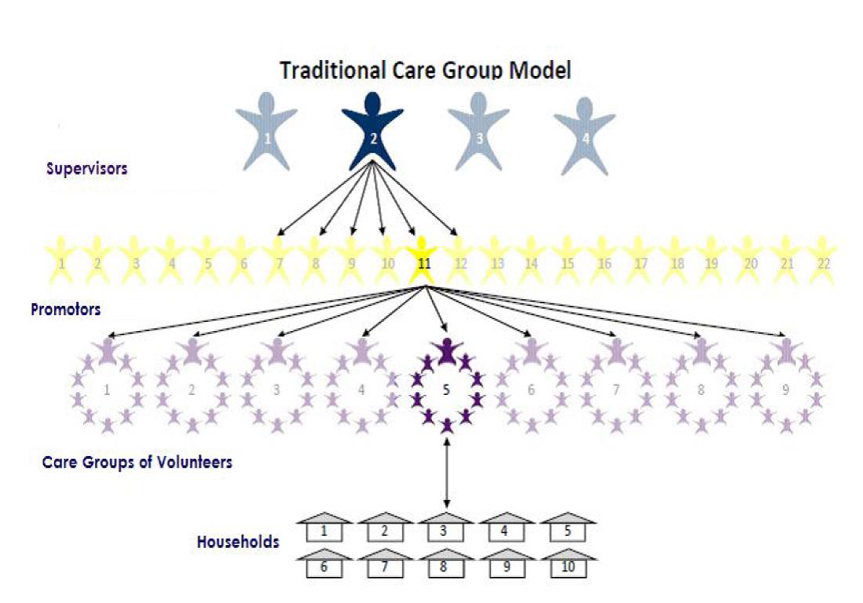
The structure of a Care Group begins with a Coordinator (paid staff) who is typically responsible for 3-6 supervisors. Each Supervisor (paid staff) is then responsible for 4-6 facilitators/promoters. Each Facilitator (paid staff) supports 4-9 Care Groups. Within each Care Group, there are 10-15 Care Group Volunteers elected by community members. Each Care Group Volunteer spreads important educational lessons to 10-15 Neighbor Women and their families, known as a Neighbor Group.
Facilitators use participatory learning through role play, songs, and skits to convey vital health messages. Care Group Volunteers report births, deaths, and other vital events to the Facilitators, which is then reported to program headquarters and used to measure the efficacy of interventions. Care Groups help reduce maternal and child mortality and malnutrition. The health messages spread by Care Group Volunteers focus on key knowledge about household practices for promoting maternal and child health, such as hand washing and other nutrition and essential hygiene actions. Care Group Volunteers also educate their neighbors on when to seek health facility services as well as pregnancy-related danger signs.*
Conclusions
Methods like the Care Group Approach are needed to expand coverage of key interventions in a cost-effective way. Impact Global Health Alliance Global has proven through multiple projects abroad that the Care Group approach is one of the best and most effective ways to mobilize and engage communities, empower women, and spread vital health education.
References:
*Perry H, Morrow M, Borger S, et al. “Care Groups I: An Innovative Community-Based Strategy for Improving Maternal, Neonatal, and Child Health in Resource-Constrained Settings.” Global Health: Science and Practice 2015; Volume 3, No. 3.
Article written by Caitlin Showalter, Programs and Development Intern



